
Effects of Anabolic Steroids on Women
Anabolic steroids, also known as anabolic-androgenic steroid hormones or simply as androgens are hormones whose major effect is masculinization. The principal masculinizing hormone that occurs naturally in men—and to a lesser extent in women—is testosterone. In fact, many of the differences between men and women are due to the higher levels of testosterone in males during development or maturity (Bardin & Catteral, 1981). Estrogens secreted by the ovaries have a major effect on fat distribution, the reproductive tract, and the pelvis. But differing amounts of testosterone account for the sexual dimorphism of nonreproductive tissues in men and women.
Only a few studies have been performed on women who take androgens because relatively few women take these drugs for therapeutic or other reasons. Thus, some of our information comes from studies of disease states in which the women themselves produce excess androgens. Also, androgens occasionally have been administered as treatment for diseases in women or, in higher doses, to masculinize female-to-male transsexuals. We also note health effects of androgens on males and surmise that similar risks may apply to females who take large amounts of androgens.
In males, testosterone is produced mainly by the testes. Its production rises dramatically at puberty and results in sexual maturity, including enlargement of the penis. Increased androgen levels, particularly testosterone levels, also result in beard growth, deepening of the voice, and coarsening of the skin. Muscle size and strength are also promoted by the presence of increased levels of testosterone (Kochakian, 1976; Kruskemper, 1968). In adulthood, differences between an eunuchoid male and a normal man are the result of the latter’s normally high levels of circulating androgenic hormones.
Women naturally have small amounts of circulating testosterone (Table 7.1). Other androgens, including dehydroepiandrosterone sulfate, are present in women in small amounts. These hormones are secreted primarily by the adrenal glands, although the ovaries also secrete a small amount of androgens. In human females, increased levels of testosterone are known to have masculinizing effects. For example, in the syndrome of adrenal androgen excess, elevated androgen secretion can result in a masculinized female before, during, or after puberty (Kochakian, 1976).
Androgenic hormones occasionally have been used therapeutically in women, usually in small doses. For example, danacrin has been used to treat endometriosis, and several anabolic steroids have been employed as antitumor agents in metastatic breast cancer (Kochakian, 1976). Side effects of anabolic steroid therapy in women may include deepening of the voice, facial hair growth, extension of pubic hair, hypertrophy of the clitoris, and loss of scalp hair (Kruskemper, 1968).
Table 7.1 Testosterone Plasma Levels and Production Rates in Men and Women
| Category | Women | Men |
|---|---|---|
| Plasma levels | 38-40 ng/dl | 700 ng/dl |
| Production rates | 0.3 mg/day | 7 mg/day |
Note: Adapted from Yen and Jaffee (1978).
In sports, men were apparently the first to use anabolic steroids in an attempt to increase strength and muscle size. However, women were not far behind. Initially, women sought to increase strength and performance in events such as the shot put; subsequently, women bodybuilders wanted larger muscles (Dayton, 1990).
Patterns of Use
The use of anabolic steroids by adolescent girls in the United States appears to be low but significant. Studies at local, state, and national levels found that approximately 1% of female high school seniors had used anabolic steroids—some as early as the 6th grade (see chapter 3).
In surveys of female intercollegiate athletes, two studies (Anderson & McKeag, 1985; Anderson, Albrecht, McKeag, Hough, & McGrew, 1991) found that 1% of participants in swimming, basketball, and track and field reported using steroids in the past 12 months. When Yesalis et al. (1990) asked female intercollegiate athletes to estimate the level of steroid use among competitors in their own sports, a somewhat different picture emerged. The respondents judged that 5% of swimmers, 6% of basketball players, and 10% of track-and-field athletes had used anabolic steroids in the past 12 months. In addition, at least one-quarter of the study participants in softball, tennis, gymnastics, field hockey, volleyball, and lacrosse believed that there was some steroid use in their respective sports in the previous 12 months.
The prevalence of anabolic steroid use is thought to be high among women engaged in bodybuilding, power lifting, shot put, and other sports that depend on maximal strength. In competitions in which drug testing has been performed, women have been detected using anabolic steroids in power lifting, bodybuilding, the shot put, the javelin throw, swimming, and running (Wadler & Hainline, 1989).
Newman (1987) surveyed elite female athletes, including those competing at the Olympic, collegiate, and professional levels in more than 15 sports. The incidence of lifetime anabolic steroids use was 3%, but only 1% of subjects acknowledged using these drugs in the preceding year. The lifetime use rates were slightly higher for those women over the age of 25 (4%) and members of professional teams (5%).
In studies of female bodybuilders conducted in Sweden (Lindstrom, Nilsson, Katzman, Janzon, & Dymling, 1990) and the United States (Tricker, O’Neill, & Cook, 1989), approximately 10% acknowledged prior use of anabolic steroids. In the U.S. study, the female bodybuilders who used steroids were younger than the male users (22 years vs. 27 years), whereas the Swedish study did not report the ages of the participants.
The levels of anabolic steroid use reported by women could be underestimates due to poor communication between the athletes and the scientists, the sanctions against drug use, or disapproval of drug use by family, friends, or fans. The virilizing effects of the drugs, and how virilization is viewed by society, also may make female athletes hesitant to disclose their steroid use.
A major question is, Do anabolic steroids help women build bigger, stronger muscles? The answer is almost certainly yes, even though no controlled studies have tested the strength of women before and after the use of anabolic steroids. This conclusion is based on the significant effects of androgen administration on muscle in female and castrated male animals (Kochakian, 1976; Kruskemper, 1968); it is also based on the physical appearance of females with adrenogenital syndrome, discussed earlier, as well as the changes in phenotype of transsexuals administered androgens.
Muscle size may decrease when steroids are stopped, although not necessarily to the pre-use level. Of course, muscle size can diminish dramatically when physical training is stopped or with disuse and inactivity.
Drugs Used
The anabolic steroids used by 10 weight-trained women athletes (Strauss, Liggett, & Lanese, 1985) are listed in Table 7.2. Oral preparations included methandrostenolone (Dianabol) and stanozolol (Winstrol). Injectable drugs included two veterinary preparations, stanozolol (Winstrol-V) and boldenone (Equipoise). The doses ranged from a moderate amount of a single drug to the use, in one woman, of five different anabolic steroids stacked during a 10-week cycle (this is comparable to moderately heavy use in the male population [Duchaine, 1989]) (Table 7.3).
Side Effects of Anabolic Steroids
Many of the side effects noted by women are a result of the masculinizing effects of these hormones. Table 7.4 lists the side effects noted by the same 10 users whose data are shown in Tables 7.2 and 7.3. Effects included
Table 7.2 Anabolic Steroids Used in Training or Competition (10 Women)
Oral
- Mesterolone (Proviron)
- Methandrostenolone (Dianabol)
- Methenolone acetate (Primobolan)
- Methyltestosterone
- Oxandrolone (Anavar)
- Stanozolol (Winstrol)
Injectable
- Boldenone undecylenate (Equipoise; veterinary)
- Methandrostenolone (“injectable Dianabol”)
- Methenolone enanthate (Primobolan)
- Nandrolone decanoate (Deca-Durabolin)
- Stanozolol (Winstrol-V; veterinary)
- Stenbolone acetate (Anatrofin)
- Testosterone cypionate
- Mixture of testosterone esters (Sustanon 250)
Note: Adapted from Strauss, Liggett, and Lanese (1985) by permission.
Table 7.3 Anabolic Steroids Reported by Heaviest User (10-Week Cycle)
| Drug | Dose | Duration of use (weeks) |
|---|---|---|
| Oral | ||
| Stanozolol (Winstrol) | 12 mg/day | 10 |
| Oxandrolone (Anavar) | 10 mg/day | 10 |
| Mesterolone (Proviron) | 50 mg/day | 10 |
| Injectable | ||
| Stanozolol (Winstrol-V, veterinary) | 50 mg/2 days | last 6 |
| Methenolone enanthate (Primobolan) | 30 mg/2 days | last 4 |
Note: Adapted from Strauss, Liggett, and Lanese (1985) by permission.
deepening of the voice, growth of facial hair, increased body hair, and enlargement of the clitoris. These effects generally appear to be permanent and have been reported by other women bodybuilders using anabolic steroids (Tricker et al., 1989). Effects that seemed to return to normal after the androgenic hormones were stopped included menstrual cessation or irregularity, increased libido, increased aggressiveness, and acne.
Of 26 female-to-male transsexuals who received long-term androgen treatment, 69% were found to have polycystic ovaries (Spinder et al.,
Table 7.4 Perceived Side Effects of Anabolic Steroids (10 Women)
| Effect | Number reporting effect |
|---|---|
| Lowered voice | 10 |
| Increased facial hair | 9 |
| Enlarged clitoris | 8 |
| Increased aggressiveness | 8 |
| Increased appetite | 8 |
| Decreased body fat | 8 |
| Diminished or stopped menstruation | 7 |
| Increased libido | 6 |
| Increased acne | 5 |
| Decreased breast size | 5 |
| Increased body hair | 5 |
| Increased loss of scalp hair | 2 |
Note: Adapted from Strauss, Liggett, and Lanese (1985) by permission.
Some women feel that menopause may be reached sooner when there is a long history of anabolic steroid use. As with men, variability exists in women’s responses to anabolic steroids (Kruskemper, 1968).
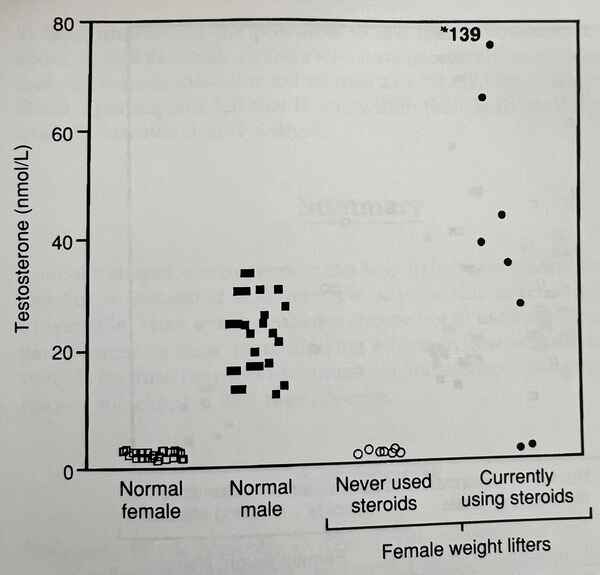
Endocrine changes have been documented. In a study of nine women weight lifters who used androgens (Malarkey, Strauss, Leizmen, Liggett, & Demers, 1991), seven women injected testosterone esters, resulting in circulating levels of testosterone up to 34 times the normal female level (Figure 7.1). Three of these seven women exceeded the upper limits of normal levels for men. The nine users of oral and injectable anabolic steroids had significantly lower levels of SHBG (Figure 7.2), thyroid-binding globulins, and HDLC as compared to controls.
The health risks that are discussed in chapter 6 apply to women as well as men. In particular, the 17-alkyl-substituted androgens are associated with liver abnormalities including (rarely) tumors. Adverse changes in lipid profiles, including decreased HDLC (Malarkey et al., 1991; Moffatt, Wallace, & Sady, 1990), suggest that women users may have an increased risk for cardiovascular disease.
If a woman was pregnant with a female fetus at the time she was taking anabolic steroids, it is likely that the fetus would be masculinized, although no cases of this have been reported.
Why Do Women Use Anabolic Steroids?
In the Strauss et al. (1985) study, the researchers attempted to analyze this question by discussing it with the subjects. All 10 women reported a significant increase in muscle strength, muscle size, and sport performance.
Figure 7.1 Serum testosterone levels were elevated in the seven women weight lifters who were injecting testosterone and were normal in the two women who were using only other anabolic steroids. Note that several testosterone levels in the women users were higher than those found in normal males.
when they first began using steroids. These were the effects that the women sought, and these effects represented the participants’ perceptions rather than objective measurements. The athletes continued to use steroids in a cyclical manner because they considered their sport performances to be better when they were taking steroids than when they were not.
Other perceived effects of anabolic steroids, including adverse effects, are shown in Table 7.4. Every athlete noticed that her voice became lower, and 7 of the 10 participants felt that this was undesirable. Nine of the 10 women observed increased facial hair, and all except one thought that this was undesirable. Eight participants noted clitoral enlargement, with no consensus as to the desirability of this change. Six noted increased libido, which most thought desirable. Breast size was believed to decrease in five subjects, four of whom attached no significance to this, and one who thought the decrease was desirable. Menstrual diminution or cessation was common, and there was no agreement as to the desirability of this.
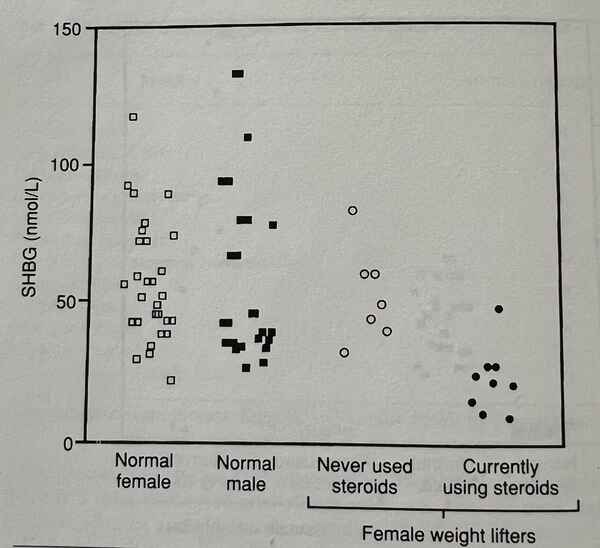
Figure 7.2 Sex hormone binding globulin levels were significantly decreased (p less than 0.02) in the women who were using anabolic steroids.
Note: Reprinted from Malarkey, Strauss, Leizmen, Liggett, and Demers (1991) by permission.
Eight women noted increased aggressiveness, six of whom felt this was desirable because it enhanced their drive to practice and compete. However, some reported that their aggressiveness caused problems in relating to associates and family members.
Nine of the women felt that athletes should not be tested for anabolic steroid use. If faced with a competition at which testing was to be performed, they would alter their drug use in an attempt to avoid detection.
The participants justified their use of anabolic steroids on several grounds. First, they felt that these drugs were necessary in order to win. Tricker et al. (1989) confirmed this perception and observed that the female bodybuilders in their study generally believed that steroids increased strength and were necessary for them to win.
Second, the side effects, although sometimes undesirable, were acceptable to the participants and their friends, husbands, or significant others. It is likely that women athletes and bodybuilders who use steroids will structure a support network that will approve of the use of these and other performance-enhancing drugs. Both males and females in this network often are lifters or athletes themselves who have used the drugs orat least understandthe pressures to use them.However, outsiders to sport, as well as female athletes who have chosen not to use steroids may look upon these masculinized women as a “Freak Show”. Finally, participants felt that it was within their individual rights to use anabolic steroids if they so wished.
Summary
Anabolic steroid use by women can help to increase muscle strength and size but is associated with multiple adverse side effects, some of them irreversible. Most women athletes choose not to use anabolic steroids, in part because of their masculinizing effects. A few women athletes use steroids because they feel that muscular and strength gains outweigh the risks or the changes that they observe.
References
- Anderson, W., & McKeag, D. (1985). The substance use and abuse habits of college student-athletes (Research Paper 2). Mission, KS: National Collegiate Athletic Association.
- Anderson, W.A., Albrecht, M.A., McKeag, D.B., Hough, D.O., & McGrew, C.A. (1991). A national survey of alcohol and drug use by college athletes. The Physician and Sportsmedicine, 19(2), 91-104.
- Bardin, W.C., & Catteral, J. (1981). Testosterone: A major determinant of extragenital sexual dimorphism. Science, 211, 1285-1294.
- Dayton, L. (1990, March). What price glory? Women’s Sports & Fitness, pp. 52-55.
- Duchaine, D. (1989). Underground steroid handbook II. Venice, CA: HLR Technical Books.
- Kochakian, C. (1976). Anabolic-androgenic steroids. New York: Springer-Verlag.
- Kruskemper, H. (1968). Anabolic steroids. New York: Academic Press.
- Lindstrom, M., Nilsson, A., Katzman, P., Janzon, L., & Dymling, J. (1990). Use of anabolic-androgenic steroids among body builders—frequency and attitudes. Journal of Internal Medicine, 227, 407-411.
- Malarkey, W.B., Strauss, R.H., Leizmen, D.J., Liggett, M.T., & Demers, L.M. (1991). Endocrine effects in women weight lifters self administering testosterone and anabolic steroids. American Journal of Obstetrics and Gynecology, 165, 1385-1390.
- Moffatt, R.J., Wallace, M.B., & Sady, S.P. (1990). Effects of anabolic steroids on lipoprotein profiles of female weight lifters. The Physician and Sportsmedicine, 18, 106-115.