
Steroids and Health Dangers
A wide variety of claims have been made about the health risks associated with the use of anabolic steroids. Many “well-established” risks are based only on anecdotal experiences and misinterpreted science. The information that is available from primary source reports of scientific studies and medical cases frequently does not support the claimed risks, but in other cases, it suggests areas of concern that have been inadequately investigated.
As researchers have gained more experience with anabolic steroids, certain parallels to the health risks associated with the use of female hormonal contraception have begun to emerge; these parallels may include consequences with long latencies, perhaps with adverse androgen effects involving the prostate or the heart. One key difference is that the health risks associated with the oral contraceptive pill are considered to be acceptable trade-offs to the prevention of pregnancy (which carries greater risks to the woman); there is, as yet, no such health benefit associated with the use of androgens by healthy young males.
Thus, the development of a life-threatening liver tumor in even one athlete as a consequence of androgen use should not be considered an acceptable trade-off for any advantage that the drug might bring in sports competition.
This chapter will evaluate the adverse effects associated with anabolic steroid use. It would be an oversimplification to reduce these risks to a single list, putting very diverse actions side-by-side with equal weight and grossly out of context. For example, the risks may range from effects that are minor in terms of well-being, such as scalp hair loss, to those that may be lethal, such as liver tumors. Risks also include temporary effects that may be useful, such as male infertility (which may become useful in male hormonal contraception), as well as temporary effects such as the profound suppression of serum high-density lipoprotein cholesterol (HDLC), for which it is difficult to rationalize any possible advantage.
An effect that is perceived as an inconvenient side effect in clinical use, such as weight gain, may be the main benefit sought by some athletes. Conversely, increasing hematocrit (another effect of steroid use) is the objective of androgen treatment of patients with severe anemia whereas the same action may predispose some individuals to polycythemia; the same potential complications are now being encountered by athletes using recombinant erythropoietin and SARM’s.
This post deals with the effects of anabolic steroid use in normal adult males, specifically the adverse effects that are produced in normally virilized men by additional androgen or by pharmacological properties of the modified anabolic steroids. This excludes some effects of virilization itself (e.g., beard growth, deepening of the voice) that are significant and undesired in a 12 year old boy or a woman.
Distinctions Between Types and Doses of Androgens
Not all androgens produce the same effects. The clearest distinction between groups of androgens is in the effects produced by the orally active steroids, most of which have been pharmacologically altered with an alkyl group at the 17-carbon position to slow their removal by the liver, and the androgens administered by deep intramuscular injection, which usually have a side chain ester at the 17β carbon position to slow their release into circulation.
According to various athlete surveys, the most popular of the 17-alkylated androgens are methandrostenolone (Dianabol), oxandrolone (Anavar), stanozolol (Winstrol), and oxymetholone (Anadrol); testosterone enanthate (Delatestryl) and nandrolone decanoate (Deca-durabolin) stand out as the most frequently injected androgen esters, and this includes their use in Olympic contestants testing positive for steroids (Catlin, Kammerer, Hatton, Sekera, & Meridink, 1987). A few exceptions to these two principal categories, such as mesterolone, testosterone undecanoate, and methenolone, so far appear to be compounds of lesser significance in the epidemiology of androgen abuse by athletes.
We should also remember that some reported adverse effects in androgen-using athletes may coincide with other common factors. For example, bodybuilders use a wide variety of drugs such as diuretics, thyroid hormone, and growth hormone in addition to steroids (Weider, 1987), and they ingest many nutritional supplements, the effects of which have been virtually unstudied. Other agents such as aromatase inhibitors may enhance adverse effects of steroids, such as a reduction in HDLC, or may actually block effects the athletes desire, such as the testosterone stimulation of growth factors .
Some effects (e.g., thrombotic stroke) may be uniquely related to the extraordinary doses used by some athletes, for whom the dose sometimes appears to be limited only by the cost and availability of the drug. At best, most athletes set their doses based on what seems to work for their friends; unlike scientifically determined doses for desired medical treatments, there is no established dose for strength or weight gain for any androgen. Some of these athletes also equate doses between different androgenic steroids by the mass units (or even more simply, by the number of tablets!), without considering differences in potency or effects.
Thus, there is no sense to the doses used by athletes, which range from levels that may be lower than replacement doses to the more frequently documented doses that far exceed any experienced in clinical medicine. For example, replacement doses of testosterone enanthate for a hypogonadal man average 75 to 100 mg/week; doses of 200 to 250 mg/week have been used in male contraceptive trials and in the treatment of oligospermia with suppression-rebound therapy; doses reportedly used by athletes for a cycle of use lasting 6 weeks or more have exceeded 1 g/week (Yesalis et al., 1988).
Oxymetholone, an orally active 17-alkylated androgen, is used at very high doses, typically 150 mg/day, to treat life-threatening anemias; this dose is comparable to that used by some athletes in conjunction with other androgens. Methandrostenolone has produced equivocal results in many studies of muscular strength effects; it is usually tested at doses of less than 15 mg/day, which is estimated to give full replacement in hypogonadal men. This drug has been administered in doses of 100 mg/day by athletes (Hervey et al., 1965), with doses up to 300 mg/day reportedly used by some athletes for several years.
Although androgens are generally used for short durations of several weeks at a time by bodybuilders, power lifters have been reported to use high doses of androgens continuously for up to 7 years (Cohen, Noakes, & Benade, 1988). Doses of such a high magnitude exert truly pharmacological effects and act through other nonandrogenic receptors or through a large increase in metabolites, which in normal concentrations would usually be unimportant.
Case Reports of Adverse Effects in Androgen-Using Athletes
One way to investigate the adverse effects of anabolic steroids is to review the medical reports of cases in which androgens are known to have been used. The publication of a case report in the medical literature depends on several factors; a physician must find out that an athlete patient has used steroids and decide that the problem may be related to this steroid use, and both the physician and a journal must be interested in publishing the case as something topical or novel.
Some athletes may conceal their drug use when complications arise, and the association may never be made. Other cases will be reported only because they are very unusual or because they involve serious illness or death. Thus, although gynecomastia is an occasional side effect encountered by androgen-using bodybuilders, there has been only one report of a series of cases from the surgeons treating this relatively minor problem (Aiachc, 1989). Clearly, this is not a suitable way to survey the problems encountered by steroid-using athletes, but it can suggest unexpected effects that bear more careful surveillance.
Suspected Disease Associations
The published case reports involving significant morbidity or mortality attributed to anabolic steroid use by athletes are summarized in Table 6.1. This summary yields some important information. For one thing, some athletes probably have died as a consequence of anabolic steroid use, but there are only a handful of such reports. In some cases in which there is a questionable association with steroid use, known causative factors of the disease were also present. For example, in addition to his history of steroid use, the 22-year-old elite power lifter with myocardial infarction weighed 330 lb and had a serum cholesterol of 596 mg/dl (McNutt, Ferenchick, Kirlin, & Hamlin, 1988).
On the other hand, the recent case investigation of a young bodybuilder who collapsed and died in the gym revealed no predisposing factors other than a damaged heart, although this could also have been explained by other factors such as a viral cardiomyopathy. These are interesting cases because several different mechanisms exist that support a potential risk of heart disease with high-dose androgen use. Other cases are simply unusual, but without further cases or a hint of a disease mechanism involving steroids, they remain enigmatic. For example, a case of a Wilm’s tumor in a steroid user has been reported.
This tumor is relatively rare, especially in adults, but it has also been observed in young adult men not known to be using any androgens. On the other hand, two cases of hepatic adenoma, also a disorder that is rare but has been observed in young men not known to be using steroids, fit into a pattern of androgen-associated tumors observed in androgen-treated patients. As such this is very likely to be a consequence of the athlete’s androgen use.
Stroke: A New Association With Androgens
Thrombotic stroke is generally unpredicted from clinical experience with androgens, but this emerges as a possible risk of androgen abuse. The three athlete cases (Frankle, Eichberg, & Zachariah, 1988; Laroche, 1990; Mochizuki & Richter, 1988) coupled with another better documented case of a young man in a hurry to mature suggest that very high doses of androgens may produce stroke. In the Nagelberg et al. case, a hypogonadal man surreptitiously increased his dosing of testosterone enanthate, achieving measured
Table 6.1 Case Reports of Significant Morbidity or Mortality in Athletes With Associated Androgen Use
| Reference | Age/Activity | Disease | Outcome | Description of androgen use |
|---|---|---|---|---|
| Prat et al., 1977 | 38 BB | Wilm’s tumor | Death from cancer with metastases | Possibly high dose methandrostenolone |
| Overly et al., 1984 | 26 BB | Hepatocellular carcinoma | Death from cancer with metastases | Many androgens for 4 years |
| Sklarek et al., 1984 | 37 BB | AIDS and hepatitis | Unknown | Shared needles in weekly steroid use |
| Goldman, 1985 | 37 BB | Hepatocellular adenoma | Surgical resection and recovery | Oxymetholone (100 mg/day for 5 years) |
| Edis & Levitt, 1985 | 27 BB | Colonic adenocarcinoma | Surgical resection and recovery | Methenolone enanthate and oxandrolone (6 months) |
| Roberts & Essenhigh, 1986 | 40 BB | Prostatic adenocarcinoma with metastases | Unknown | 15 cycles of many androgens in 20 years |
| Creagh et al., 1988 | 27 BB | Hepatocellular adenoma | Death from hemorrhage | Anabolic steroids for at least 3 years |
| Frankle et al., 1988 | 34 BB | Cerebrovascular thrombosis | Partial recovery | Cycles of anabolic steroids for 4 years |
| Mochizuki & Richter, 1988 | 32 BB | Cerebrovascular thrombosis (?) and cardiomyopathy | Partial recovery | Many androgens since age 16; stopped 4 months before second stroke |
| McNutt et al., 1988 | 22 PL | Myocardial infarction | Recovery | Intramuscular and oral androgens for 6 weeks |
| Scott & Scott, 1989 | 26 BB | AIDS | Unknown | Repeatedly shared a needle with infected BB injecting steroids |
| Luke et al., 1990 | 21 BB | Sudden cardiac death | Death | Injected nandrolone and testosterone esters |
| Laroche, 1990 | 28 BB | Cerebrovascular and peripheral thromboses | Recovery | Monthly injections of many steroids for 3 years |
| Winwood et al., 1990 | 30 PL | Bleeding esophageal varices | Recovery | Stanozolol, oxandrolone, and methandrostenolone for 18 months |
Note: BB = bodybuilder; PL = powerlifter. Adapted and updated from Friedl (1990).
plasma testosterone concentrations of over 100 ng/ml, or 10 times normal levels. At least one of these cases was clearly identified as a cerebrovascular and peripheral thrombosis (Laroche, 1990), and several cases of thrombotic stroke have been reported in Japanese males receiving large doses of oxymetholone or fluoxymesterone for treatment of hypoplastic anemia.
Clotting abnormalities can be produced by some androgens but the reported effects are inconsistent, with an increase in clotting factors produced by some androgens; other reports suggest an increase in fibrinolytic activity.
The connection may be through an estrogen effect, achieved when high doses of androgens also produce elevated estrogen levels; increased estrogenicity is supported by the occurrence of gynecomastia in some androgen using athletes, including two of the athletes with stroke. This connection is suggested by the increased risk of thrombotic stroke observed in young women taking oral contraceptives (Collaborative Group for the Study of Stroke in Young Women, 1975) and the increased risk of thromboembolism (without change in myocardial infarction rates) in male patients treated with estrogens (Coronary Drug Project Research Group, 1973).
Prostate: An Androgen Target and Potential for Disease
Some other potential risks of steroid use require special vigilance. The androgen parallel to breast cancer risk from the oral contraceptive pill may be prostate cancer, because the prostate is a target tissue for androgens and the cancer is androgen sensitive. Prostate cancer can be induced in some special strains of rats after several months of androgen treatment (Noble, 1984), but no such connection has emerged for man after nearly 4 decades.
However, established prostatic cancer is generally treated by reduction or complete blocking of androgens, and the disease is worsened with testosterone administration, even in men who have not responded to the hormonal therapy . One study suggested that the high rate of prostate cancer in black males is linked to a purportedly higher resting testosterone level , but in the same theoretical terms we can argue that the risk is reduced with androgen use because sex hormone-binding globulin, which is higher in patients with prostatic carcinoma, is reduced by anabolic steroids.
There is no evidence of prostate stimulation from any of the male contraceptive studies using doses of androgens up to 200 mg/week for more than 12 months . The one case report of prostate cancer in a white bodybuilder who, at 40, was unusually young for this disease is useful only as a reminder of what may emerge as today’s androgen abusers grow older (Table 6.1).
Musculoskeletal Injuries
Another group of case reports involves musculoskeletal injuries, which so far cannot be distinguished from the risks ordinarily faced by strength athletes with extraordinary muscle hypertrophy, even those who don’t use anabolic steroids. The suggestion of an association comes primarily from animal studies by Michna (1987) in which methandrostenolone injected into exercised mice produced collagen abnormalities; this has been interpreted as a change that might increase the risk of tendon rupture.
Diseases Indirectly Associated With Androgens
Infection with AIDS and other types of infection are risks of the use of contaminated needles or contaminated black-market products also associated with androgen use. The wide variety of doses, drug combinations, supplements, and other drugs used by athletes makes it difficult to pinpoint the agent responsible for an adverse effect.
Nearly all of the medical case reports involve bodybuilders, suggesting that steroid-using bodybuilders far outnumber all other athletes combined, that bodybuilders use the drugs in ways that put them at greater risk for health consequences (e.g., higher doses, longer duration, or use with other drugs), or that bodybuilders are proportionately more likely to be in the known high risk groups for AIDS. Unfortunately, no systematic study of the medical risks of androgen use by any athletes has ever been conducted and even the population of adult athletes at risk remains poorly defined.
More reliable information on androgen effects is available from male contraceptive trials, in which greater than replacement doses of androgens have been tested for durations at least as long as typical user cycles, and from therapeutic treatment of specific diseases, such as aplastic anemias with high-dose androgen treatment and male hypogonadism with replacement dose treatment. Even replacement dose treatments yield adverse effects because of pharmacological properties of the synthetic steroids (such as 17-alkylation), and some of these effects will be common to androgen-abusing athletes. These known or suspected health consequences of androgen use can be divided into five main categories:
- cosmetic effects,
- heart disease,
- liver toxicity,
- liver tumors, and
- infertility.
The remainder of this post will focus on these five areas.
Cosmetic Effects
Among the best-known side effects of androgen use in athletic circles are the cosmetic actions that include oily skin and acne, changes in hair patterns, and gynecomastia. Athletes have seen these effects with some frequency either in themselves or in others around them. One of the reasons that these effects are so well acknowledged is that they are visible effects that an appearance-conscious bodybuilder may especially dread.
Effects on Hair
Body hair patterns are steroid hormone dependent, and normal virilization includes increased facial hair growth and a gradual recession of the temporal hair line. Castration can prevent or arrest baldness in men, and treatment of castrate men with androgens again permits scalp hair loss. Thus, it is assumed (but has never been studied) that balding is accelerated with long-term androgen administration to normal individuals with such a genetic predisposition. Contraceptive studies lasting for up to several months have reported only slight increases in hair on the chests, backs, or lower abdomens of some subjects.
Acne
The studies of castrate men have also shown that acne is dependent on male sex steroids, because it does not occur in men castrated early in life but can be induced in some eunuchs with testosterone propionate treatment. The appearance of mild truncal acne or folliculitis has also been reported in male contraceptive studies involving greater than replacement doses of testosterone enanthate and with use of methyltestosterone . Pharmacological doses of androgens increase sebaceous gland size and secretion rates , and even relatively weak androgens can markedly increase sebum
production . These effects have also been demonstrated in athletes treating themselves with high-dose androgens, and a specific increase in skin lipid cholesterol content has been reported (Kiraly, 1988). This increased synthesis of the cholesterol component is thought to appear at peak levels in the sebum excretion after 3 to 4 weeks of androgen administration.
Gynecomastia
Gynecomastia, the development of abnormal breast tissue in males, is another benign cosmetic disorder that is a well-recognized but poorly understood consequence of androgen use in athletes . Transient gynecomastia or some of the early symptoms have also been occasionally reported in male contraceptive studies. This disorder occurs in men when estrogen levels increase or androgen levels decrease relative to the amount of estrogen present.
Estradiol is a potent hormone that causes this effect, and once established the gynecomastia may persist, even after the initial stimulus is gone; thus, the effect may not be directly traceable to an elevated estradiol level. In rare cases, gynecomastia may be a direct consequence of the use of potent estrogens by male bodybuilders who apparently will add anything labeled “steroid” to their polypharmacy repertoire.
Gynecomastia has been reported in men with various liver diseases, including alcoholic cirrhosis and hepatocellular carcinoma, and it is a common occurrence during male pubertal maturation. Gynecomastia has been occasionally reported in clinical applications of androgens and in male contraceptive studies, but it has always been observed as a mild and transient phenomenon that eventually ceases even with continued steroid treatment.
Bodybuilders have tried to prevent or treat gynecomastia with estrogen blockers and by using other androgens that may be less likely to convert to potent estrogens, but these solutions usually do not provide clear relief; for the most severe cases, surgical removal of the excess breast tissue is cosmetically necessary.
Heart Disease
Heart disease is a much discussed risk of anabolic steroid use, but it is an outcome which remains to be demonstrated. There are good reasons to believe that longterm abuse of anabolic steroids will increase the incidence of heart disease in users over nonusers, but there is no epidemiological data to suggest that this actually happens.
Serum Lipids
One of the most well-established adverse effects of androgen self-administration by athletes is the reduction in serum HDLC (Figure 6.1). However, even though this finding seems incontrovertible, reduced HDLC is not a necessary consequence of androgen use because not all androgens produce this effect. Nevertheless, most athletes use the orally active compounds that produce this effect, either by themselves or in addition to injectable steroids, and no study of self-administration by athletes has failed to report a significant decline in HDLC. HDLC levels begin to decline within a few days after the start of use and can recover within approximately a month after cessation, although this probably depends on the rate of steroid elimination.
This reduction in HDLC is due to a stimulation of a liver enzyme that regulates serum lipids, hepatic triglyceride lipase. Stimulation of this enzyme leads to a reduction primarily in the HDL-2 cholesterol subfraction and its accompanying apolipoprotein-A1. This reduction can be profound, and in several of the
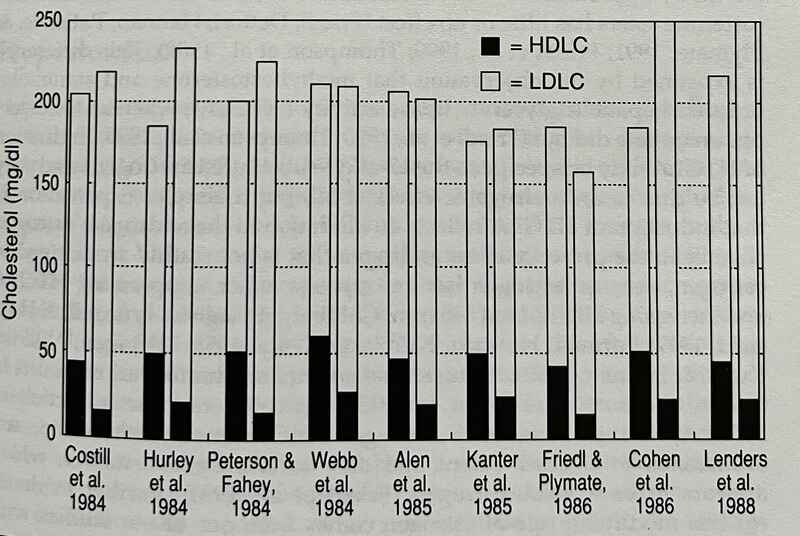
Figure 6.1: Serum lipid measurements without and with androgen self-administration in athletes. The decline in HDLC with androgen administration is consistent across studies, whereas total cholesterol increased significantly in two of the studies. All the studies used 17-alkylated androgens with or without injectable androgens. Note: Adapted from Friedl (1990).
lipid surveys, HDLC concentrations in the single-digit milligram-per-deciliter range have been observed for some of the athletes. By itself, this reduction in HDLC is considered a risk factor for coronary artery disease . For middle-aged men studied in the Framingham Heart Study who had levels of 25 mg/dl compared to men with initial levels of 50 mg/dl, the risk of developing heart disease was tripled.
Although a few studies have also reported increases in total cholesterol, this has not usually been observed. Instead, the decrease in circulating HDLC appears to be generally offset by the same magnitude of increase in low-density lipoprotein cholesterol (LDLC), with no net alteration in total cholesterol.
The HDLC depression observed so consistently in self-medicating athletes is not an obligatory consequence of androgen use. The substantial HDLC reduction produced by methyltestosterone in early androgen studies was actually proposed for use as an index of androgenic potency ; however, subsequent studies in normolipid subjects have failed to demonstrate a clinically significant reduction in HDLC with androgen ester administration in doses that are markedly androgenic. Thus, although 17-alkylated androgens reduce HDLC by approximately half, the administration of nandrolone and testosterone esters has little or no effect.
This difference is explained by the observation that methyltestosterone and stanozolol induced hepatic triglyceride lipase activity (HTGLA), whereas testosterone enanthate did not. Induction of HTGLA may be specific to the 17-alkyl-substituted androgens and may not be due to an androgenic effect at all, but a simpler explanation is that induction of HTGLA reflects an alteration in the androgen/estrogen balance in the presence of an androgen that is not readily aromatized to estrogen, because estrogen has an opposite effect, suppressing HTGLA and increasing HDLC.
Testosterone enanthate administration results in a large increase in estrogen and this can counteract the induction of HTGLA, whereas some other androgens, such as methyltestosterone, are aromatized to a lesser extent and only to 17α-methylestradiol, which appears to be a weak estrogen. Further evidence for this modifying role of estrogen comes from one of our studies with coadministration of the aromatase inhibitor testolactone with testosterone enanthate.
This suppressed the normally observed increase in estradiol following administration of the enanthate and produced a modest but significant reduction in HDLC that did not occur with testosterone enanthate alone. This means that the estrogen inhibitors that some bodybuilders use along with their androgens in an attempt to prevent gynecomastia may enhance the suppression of HDLC.
Glucose Tolerance
Hyperinsulinemia and impaired glucose tolerance have been reported with use of methandrostenolone and oxymetholone and for athletes self-administering several androgens. Such an effect may adversely affect serum HDLC, and researchers have suggested from epidemiological observations that testosterone increases risk of heart disease through an effect on insulin. Alternatively, glucose intolerance may count as an additional independent risk factor, additive to the risk associated with HDLC reduction. This effect has not been duplicated with androgen esters ( or with injected methenolone acetate, a 1-methylated androgen (Landon et al., 1963). In fact, androgen administration to normal men has recently been demonstrated to improve glucose disposal.
Hypertension
Hypertension is perhaps one of the most exaggerated claims of androgen-associated health risks. This claim appears to have originated in a position statement (ACSM, 1987), and this has since been quoted to athletes around the country.
This position paper referenced a review article on high blood pressure that was based on a single study of weight lifters. In that study, athletes given methandrostenolone (10 to 25 mg/day for 6 weeks) were reported to show slight pre-post increases in systolic blood pressure, and one of the men “tended to be hypertensive on the drug”. However, this observation has never been confirmed.
Subjects given a substantially higher dose of methandrostenolone—100 mg/day—for 6 weeks demonstrated no changes in blood pressure, and none of the half-dozen or more strength studies that have involved administration of 5 to 20 mg of methandrostenolone per day to men have found such an effect. In a study that also reported an increase in blood pressure, the average systolic pressure was 118 mm Hg before and 121 mm Hg after 8 weeks of steroid self-administration by a group of amateur bodybuilders (Lenders et al., 1988); this was reported as statistically significant, although in practical terms this difference is meaningless.
No other studies have reported a change in blood pressure, even though some have specifically tested it in athletes who self-administer steroids and in controlled studies with high-dose androgen administration. Thus, although androgens can theoretically affect blood pressure in some susceptible individuals through a mechanism analogous to that observed with oral contraceptives, it is not a well-established action.
Alterations That May Reduce Cardiovascular Risk
Androgen-induced alteration may actually reduce other health risk factors. For example, stanozolol administration has been shown to reduce the serum lipoprotein-(a), which may signify a reduction in the risk of ischemic heart disease and cerebrovascular disease. Other characteristics of steroid-using male athletes tend to put them in a low-risk group for heart disease. While they are engaged in athletics, these men tend to exercise intensively, maintain relatively low body fat, and avoid smoking. Thus, whether or not the temporary serum lipid changes produced by 17-alkylated androgens produce a real difference in an eventual heart disease outcome in these athletes remains to be established.
Cardiomyopathy
At least one study has suggested that injected methandrostenolone can cause myocardial damage in guinea pigs, although exercising these animals produced similar changes. Case reports have also suggested that anabolic steroids increase left ventricular mass beyond that which can be attributed to hypertrophic responses in strength athletes not using steroids. McKillop, Todd, and Ballantyne (1986) reported an extraordinarily large but not necessarily pathological heart in a 23-year-old bodybuilder who had used steroids intermittently for 8 years.
His ventricular wall thickness of 27 mm far exceeded the upper limits measured in 947 elite athletes. However, the role of androgen use in this hypertrophy cannot be determined, and at least two studies comparing strength athletes who use steroids with those who do not have failed to detect a difference in left ventricular size.
To date there are only two published cases of heart disease in young androgen-using athletes. As previously described, other predisposing factors were present in the survivor. The most recent case, which resulted in death, revealed an extensive myocardial fibrosis at autopsy.
Postmortem samples from the athlete tested positive for nandrolone metabolites; vials of nandrolone and testosterone esters and a potassium supplement were found in his gym bag. The authors appropriately pointed out that this death could be simply the consequence of a viral or toxic myocarditis or it could be directly related to a steroid-induced cardiac pathology, through any of several potential mechanisms. These could include serum lipid changes, platelet hypercoagulability, a heightened vascular response to norepinephrine, and coronary vasospasm; however, no data were collected that suggested any of these factors were altered. Another case that was reportedly investigated demonstrated a familial risk: The father of a 27-year-old steroid user who died of heart disease had died at age 32 of heart disease. If there is an increased incidence of heart disease in androgen-using athletes, it is likely to be detected only in a properly designed epidemiological study with careful control of the potential confounders.
Liver Toxicity
Many pharmacological actions of steroids center on the liver. This is a target tissue for androgens and also a principal site of steroid clearance. If the main route of drug delivery is by ingestion, then the liver will also be exposed to the full dose arriving via the portal vein before it is further distributed in the circulation. The actions range from effects on specific proteins such as hepatic triglyceride lipase and sex hormone-binding globulin, to stimulation of hepatocyte hypertrophy and even the formation of benign tumors. At least in patients with already compromised hepatic function, the imposition of high doses of some orally active anabolic steroids has been demonstrated to produce cholestasis and may produce other forms of liver damage.
Liver Enzymes
Few reviews on anabolic steroids have failed to highlight the alteration of liver function tests that is frequently observed following administration of 17-alkylated androgens; however, this effect appears to be much overrated. Moderate increases in serum activity levels of these enzymes have also been observed in androgen-using athletes, but even with significantly higher values than control subjects or over-baseline values, serum activity levels tend to remain in the normal range. When enzyme levels such as serum glutamate oxaloacetate transaminase (SGOT) exceed the normal range in steroid-using athletes, this may be a reflection of skeletal muscle damage from intense training (and from steroid injections) rather than a reflection of specific liver tissue damage.
In patients the elevation has been reported to be a transient phenomenon even with continued use. Petera, Bobek, and Lahn (1962) found that methyltestosterone (30 mg/day) produced a peak rise in both SGOT and glutamate pyruvate transaminase levels after approximately 10 to 12 days of administration to 40 patients, and with continued therapy, the levels declined again. This is consistent with the observation that there was no change in liver function tests at 1, 2, or 3 months of oral methyltestosterone administration (40 mg per day) to normal men.
Furthermore, Petera et al. (1962) found that the transient enzyme elevation was associated with 17-alkylation; no change occurred if patients were treated with testosterone propionate (25 mg/day), either by oral or parenteral routes of administration. Oral testosterone given to normal men in four 100-mg doses per day also did not change any liver function tests over 21 days also found increased serum transaminase levels only with 17-alkylated androgens and no increase with testosterone propionate or even with an orally administered 1-methylated androgen. The pathological significance of this transient increase remains unknown.
Cholestatic Jaundice
Cholestatic jaundice has been noted in some patients treated with 17-alkylated androgens; usually this has involved individuals who are being treated for very serious diseases. There have been no reports of androgen-using athletes with this problem. This may be because athletes usually do not use the androgens that have been associated with this effect, because athletes stop using androgens on their own when they become icteric, or because jaundice is dismissed as a well-known consequence of androgen use and is not reported by treating physicians.
The first suggestion that some androgens might cause liver problems came when physicians tried to treat patients with methyltestosterone for the severe itching associated with obstructive jaundice; the jaundice worsened in most of the treated patients.
This, and several cases of jaundice in hypogonadal men replaced with methyltestosterone, led to the association of cholestatic jaundice with 17-alkylated androgen administration. Nearly every report has been of patients treated orally with 17-alkylated androgens, usually involving methyltestosterone or norethandrolone, but also including stanozolol, methylnortestosterone, and methandrostenolone. A single case report of jaundice with testosterone enanthate administration was described for a pregnant woman, but this cannot be distinguished from pregnancy-related jaundice that occurs in some women.
The frequency of cholestasis in patients treated with high doses of androgens ranges from a few patients demonstrating some histological evidence of disease to 17.3% of patients developing an overt jaundice. This form of cholestatic drug reaction generally lacks histological features of inflammation and necrosis and is characterized by an accumulation of bile in cells and canaliculi. Recovery typically occurs within several weeks after drug cessation, and jaundice does not necessarily recur in these patients with reinstitution of treatment. Death is a highly unlikely consequence:
The reported deaths caused by cholestatic jaundice have all occurred in elderly or very ill patients, including two patients with metastatic carcinomas and at least one suspected of suffering from severe viral hepatitis. In four of these cases, the medication was continued until the death of the patient because it was not recognized as (nor was it necessarily) the cause of the cholestasis.
Intrahepatic cholestasis can be produced with norethandrolone infusion in rats, and the primary defect appears to be a disruption of microfilaments similar to the action produced with cytochalasin B. This suggests that reduced bile transport and hepatocyte structural changes that lead to cholestasis are mediated through this single mechanism.
Reduced transport may be an early marker of hepatic dysfunction because it appears to precede cholestasis and jaundice. In a large study with anemia patients given one of four oral androgens (norethandrolone, methandrostenolone, oxymetholone, and the 6-methylated methenolone), 35% of patients had signs of abnormal liver function, including reduced bromosulfophthalein (BSP) uptake, and half of these had overt jaundice.
In another study, abnormal BSP retention was noted in 74% of 47 patients treated with norethandrolone (25 or 50 mg/day), but liver biopsies from seven of the patients with poor BSP retention times yielded normal tissue, with only one demonstrating a minimal bile stasis and focal necrosis. Hypercholesterolemia is also a marker of cholestasis, and the reportedly high cholesterol levels in one study of androgen-using athletes are conceivably related to such liver dysfunction.
Peliosis Hepatis
Peliosis hepatis is a potentially life-threatening hepatic lesion characterized by a spectrum of microscopic to grossly visible blood-filled cysts in the liver. Although peliosis hepatis was originally recognized as a very
Table 6.2 Case Reports of Deaths Attributed to Androgen-Induced Cholestatic Jaundice by the Reporting Authors or Later Reviewers
| Reference | Age/sex | Disorder treated | Androgen/dose/exposure | Cause of death |
|---|---|---|---|---|
| Koszalka, 1957 | 60 M | “To improve healing and protein anabolism” (metastatic disease) | Methyltestosterone (sublingual) 30 mg/day, 10 weeks | “Obstructive jaundice” |
| Peters et al., 1958 | 62 M | “Therapeutic trial” (metastatic disease and angina, treated with I131-induced myxedema) | Methylnortestosterone 6-25 mg/day, 18 weeks | ?(Histology: “resolving jaundice”) |
| Gordon et al., 1960 | 43 M | Corticosteroid-induced osteoporosis | Norethandrolone 30 mg/day, 23 weeks | Cholestasis and peliosis |
| Gordon et al., 1960 | 57 F | Anorexia (result of “pancreatic insufficiency”) | Norethandrolone 20 mg/day, 42 weeks | “Severe viral hepatitis” with cholestasis and peliosis |
| Gilbert et al., 1963 | 74 M | Osteoporosis and hemiplegia | Norethandrolone 30 mg/day, 30 weeks | Sepsis and intrahepatic cholestasis |
Note: Reprinted from Friedl (1990).
rare disease associated almost exclusively with pulmonary tuberculosis, a relationship between peliosis hepatis and androgen treatment was proposed in 1952. Since then, more than 70 cases of hepatic and splenic peliosis have been reported in association with androgen administration. In autopsies of Japanese patients with aplastic anemia, 7 of 19 patients who had been treated with oxymetholone or methenolone had peliosis, compared to only 1 of 28 patients not treated with androgens.
In an American series, 5 out of 9 patients treated with androgens for wasting diseases had peliosis at autopsy. In healthy patients, peliosis may not be as prevalent. Out of 60 transsexual women and impotent men treated with methyltestosterone (150 mg/day) for up to 5 years, nine patients had sinusoidal dilatation and three patients had cyst formation, suggestive of potential prepeliosis lesions. Although the patients in this series were free of symptoms, a later case report described peliosis hepatis and liver tumor rupture requiring emergency surgery in one of the transsexuals following 7 years of continuous androgen treatment.
In a 3- to 5-year follow-up of many of the patients from this series and others who were administered various androgens, Lowdell and Murray-Lyon (1985) found hepatic abnormalities (based on liver scans and colloid uptake) only in the patients still using methyltestosterone, with resolution of abnormalities in those who had stopped using methyltestosterone, and essentially normal livers in those administering their steroids lingually or parenterally.
Most of these reported peliosis cases involve patients treated with 17-alkylated androgens, including fluoxymesterone, norethandrolone, oxymetholone , methenolone, and methyltestosterone. Peliosis is not clearly associated with androgen esters. Postmortem examinations of 52 dialysis patients treated with testosterone enanthate (up to 250 mg/week for 5 months) revealed no peliosis; however, another postmortem study revealed peliotic lesions in six chronic renal failure patients who had received only androgen esters for an average of more than 3 years.
Peliosis has also been observed in a woman treated with tamoxifen, a drug that is also used by some androgen-abusing athletes in an attempt to prevent gynecomastia. Although this represents only a single case, it is unusual because peliosis is such a rare disorder and this case may indicate a role of an androgenic/estrogenic component in this disorder.
Peliosis may not be readily diagnosed by standard laboratory studies, and it is usually discovered either as occult disease in postmortem examination or, rarely, as a result of symptomatic hemorrhage. At least five patients have died from internal hemorrhage resulting from their peliosis, but internal hemorrhage is also a frequent cause of death in severe anemias. Several cases of death from hepatic failure have also been attributed to an existing peliosis, although in some of these cases metastatic disease and severe cholestasis may have been more directly responsible for patient death. One case of histologically diagnosed peliosis hepatis was followed after androgen withdrawal, and complete recovery was observed.
Mechanism of Cholestasis and Peliosis Hepatis
A single mechanism has been proposed to explain the occurrence of both cholestasis and peliosis hepatis. Based on microscopic evaluation of biopsy material from the Westaby series of patients treated with methyltestosterone, it has been proposed that 17-alkylated androgens specifically produce hepatocyte hyperplasia; the enlarged hepatocytes then encroach on the hepatic venous system occluding vessels and perhaps also blocking bile canaliculi to produce cholestasis, peliotic sinusoids, and perhaps even esophageal varices.
Liver Tumors
Several diseases, including heart disease and hepatocellular carcinoma (HCC), occur with higher frequency in males than in females. Thus, androgen links to heart disease and HCC have been extensively investigated. Animal studies with castration and androgen replacement support a connection with HCC. However, androgens are not mutagenic in the Ames test; instead, they appear to promote tumor formation by enhancing the effects of carcinogens. Androgen doses that are 400 to 600 times the human clinical dose, given over the life span of a rodent, usually cause liver growth (hypertrophy and hyperplasia) but without tumors. In mice, 6 weeks of treatment with nandrolone decanoate (600 mg/kg/week) did not produce liver tumors, but following exposure to dimethylnitrosamine, which is known to produce liver cancer in this model, the expected tumor formation was further enhanced.
Characteristics of Androgen-Associated Liver Tumors
There is little question that administering androgen to men increases their risk of liver tumors. The type of tumor that is promoted appears to act more like a benign hepatocellular adenoma (HCA), which rarely occurs
in men, than like the malignant HCC, with which it shares some diagnostic features . The principal distinction between the diseases is reflected in the aggressive behavior of the typical HCC; the median survival time for patients with HCC may be as short as 1 month, with very few patients expected to live beyond 1 year (Peters, 1976), whereas the androgen-related tumors in some individuals have regressed following androgen withdrawal, and even have regressed in some individuals without any other treatment.
Nevertheless, benign should not be interpreted to mean non-life threatening, because at least several of the androgen-related cases have been diagnosed as a result of tumor rupture and serious internal bleeding, even culminating in the death of one bodybuilder.
Since a relation between androgen treatment and hepatic tumors was first suggested, at least 91 cases of androgen-associated tumors have been reported in the medical literature. Nearly half of these have been diagnosed in patients with an inherited form of severe anemia (Fanconi’s anemia) who were treated with androgens.
Hereditary anemias such as Fanconi’s syndrome carry an increased incidence of malignant neoplasia, and patients with such anemias may be predisposed to the development of hepatic tumors, with such tumors emerging more frequently when lives are extended by androgen therapy. However, at least 43 of these cases are not Fanconi’s patients and include definitive diagnoses based on microscopic evaluation of tumor material obtained from the patients.
After we eliminate cases in which hepatic tumors were not the cause of death and were detected only at autopsy, and several diverse diagnoses involving hepatic angiosarcoma and focal nodular hyperplasia, a large set of cases that are variously diagnosed as HCA or HCC remains. These cases collectively exhibit characteristics that can be described as very unusual for tumors that look histologically malignant; with the common connection of androgen use, they suggest a peculiar androgen-specific form of liver tumor (Anthony, 1975). This is now recognized as a distinct form of liver tumor (Craig et al., 1989).
The earliest known case with an androgen association (Drew, 1984) typifies the liver tumors that this section has described. In 1961, hepatocellular carcinoma was diagnosed in a 44-year-old man presenting with a right upper quadrant abdominal mass. Part of the tumor was removed and he was given chemotherapy. Twenty-two years later, this patient was still alive with no complaints of liver dysfunction. The unusual characteristics of this HCC include the long survival following diagnosis, the absence

Figure 6.2 Anabolic steroid–associated hepatocellular adenoma, now recognized as a diagnostic category of benign epithelial tumors. The top view shows a 9-cm diameter hepatocellular adenoma from a patient with Fanconi’s anemia who was treated with methyltestosterone for 4 years; the bottom view shows a cross section of the tumor. Note: Reprinted from Craig, Peters, and Edmondson (1989).
of metastases, and the absence of elevated alpha fetoprotein production. Nearly all of the reported cases are also negative for serum hepatitis surface antigen and lack evidence of an associated cirrhosis, which is found with many of the more typical HCC cases, in the absence of known exogenous androgen exposure (Peters, 1976). That these cases are androgen related is supported by the finding that tumor regression occurred in more than half of the cases with follow-up observation following androgen withdrawal, with no other treatment (or only partial tumor excision).
Most of these cases involved patients who were being treated for androgen deficiency (usually with methyltestosterone, at a typical dose of 50 mg/day) or for severe anemia (usually with oxymetholone, at a typical dose of at least 100 mg/day). Only two cases were associated with exclusive use of androgen esters.
Liver Tumors in Athletes
The three most recent case reports comprise all the reports of liver tumors in androgen-using athletes. These include one patient who died from a metastatic carcinoma, one who died from internal hemorrhage following the rupture of an adenoma, and another who apparently survived following surgical removal of an adenoma. In the case reported by Overly et al. (1984), the features are typical of the better known malignant hepatocellular carcinoma, including high serum levels of alpha fetoprotein synthesized by the carcinoma, and the aggressive biological behavior of the tumor with metastasis and short time to death. This case also included cholangiole involvement, seen in only two other patients in these cases (one of which also metastasized). Thus, this cancer case does not bear the characteristics typical of the androgen-associated tumors.
Vascularization of the Tumors
The apparent likelihood of tumor rupture in the case reports of androgen-associated tumors is independent of the tendency to develop peliosis. In these patients, peliosis was not consistently present with the tumors (it was described in half of the cases), and it has been suggested that necrotic lesions described as peliosis may be more accurately represented as vascular ectasia, frequently seen with tumors. As an example, in the case of the athlete who died following tumor rupture, the liver surrounding the adenomas was described as hyperplastic with ectatic sinusoids but was apparently devoid of peliotic cysts.
Certainly, the case reports emphasize symptomatic patients who were brought to medical attention, and the reports are submitted for publication because of the severity of the problems; 24 out of 28 androgen-related HCA or HCC case reports involved acute abdominal pain or internal hemorrhage. The majority of androgen-associated tumors may remain undetected because they do not rupture and the patients remain asymptomatic, such as the cases of such occult diseases that have been described from careful postmortem examinations of androgen-treated patients.
On the other hand, in 31 cases of hepatocellular adenoma in males collected from the literature, all three tumors associated with androgen use ruptured. We can also hypothesize that 17-alkylation does not produce more tumors than the androgen esters but simply increases the likelihood of discovery through rupture; described tumors and peliosis associated with nonalkylated androgens in a mostly postmortem series.
Androgens are likely to increase the risk of hemorrhage in individuals with liver tumors through an effect of increased fibrinolytic activity; this has been reported in patients receiving either oral androgens (Fearnley & Chakrabarti, 1962) or testosterone propionate, but only some 17-alkylated androgens (including oxymetholone) have been found to decrease fibrinogen. The high rate of adenoma rupture and hemorrhage in women using oral contraceptives, compared to women with HCA not using oral contraceptives, is particularly associated with the use of 17-alkyl-substituted progestagens. These data suggest a structural specificity; although, this too, can reflect selective reporting.
Incidence of Androgen-Associated Liver Tumors
The occurrence of androgen-related tumors appears to be considerably higher than the rate of hepatic tumors associated with female oral contraceptive steroids. Within 5 years of the first case report associating oral contraceptives with liver tumors, at least 117 cases had been documented in the literature, with perhaps 100 more claimed; 92% of these cases involved benign tumors, for which less than 400 cases had been reported in women since.
Oral contraceptive–related tumors are rare relative to the size of the population at risk; at least 30 million women in the United States alone are estimated to be currently using contraceptive steroids. The prevalence of androgen use, even including use by androgen abusers, is not reasonably expected to come close to this, nor is exposure during the past 30 years likely to rival oral contraceptive exposures, yet the literature already documents nearly 100 cases of androgen-associated liver tumors.
In patients with severe anemia who survived 2 years with androgen treatment, the incidence was two benign tumors in 137 patients ; previously, a case with tumor rupture was reported for a patient from the larger sample of 429 patients originally enrolled in the same series (in which 3 of the 429 patients had tumors), although many of these additional patients had a shorter exposure to androgens.
In a series of 60 female-to-male transsexuals and impotent men treated with high-dose methyltestosterone only one HCA was detected, although another case with tumor rupture was later reported for a transsexual from the same series (in which 2 of the 60 patients had tumors). Thus, the incidence of hepatic tumors may be estimated to be 1 to 3% within 2 to 8 years of exposure of greater than replacement doses of 17-alkylated androgen; occult disease is likely to also be present and makes this incidence higher.
Another rare form of liver cancer, hepatic angiosarcoma, was also associated with androgen use in a retrospective epidemiological study. In a review of 168 cases of histologically confirmed cases of hepatic angiosarcoma, researchers identified four cases with some previous androgen exposure (3.1%) from a review of medical records. The connection with androgen exposure remains unconfirmed with no new androgen-associated cases reported since the latest of the four case deaths in 1974, and at least one of those four patients was exposed to isoniazid, another proposed agent of hepatic angiosarcoma.
Three cases of focal nodular hyperplasia have been reported in patients with androgen exposure, in two cases with only 3 and 6 months of androgen exposure, also leaving the role of androgen open to question.
Infertility
Male athletes who self-administer high doses of androgen are likely to be infertile during their period of use and for some time, perhaps as long as 6 months, after cessation of use. This effect cannot be reliably produced in all males, and not all androgens are equally effective in this action. No cases of irreversible infertility as a result of androgen administration have ever been reliably documented, although athletes using these androgens are naturally concerned when they notice a shrinking testicular volume, which usually accompanies the temporary reduction in testicular stimulation by trophic hormones and the depletion of developing germ cells.
Spermatogenesis is markedly suppressed in athletes using a wide assortment of androgens. In a study of bodybuilders, the average sperm count of the men who had used steroids within the past 3 months was less than 20 million/ml, whereas those who had stopped their use for 4 to 24 months prior to the count averaged 84 million/ml. The researchers observed no difference between fertile control subjects and these steroid users regarding the proportion of sperm motility or abnormal morphology, suggesting that these other parameters may be unaffected.
Controlled Trials of Reversible Male Contraception
Many controlled studies have examined the effect of high-dose androgen administration to fertile males to test the suitability of male steroidal contraception. The oral androgens, such as methyltestosterone and testosterone undecanoate, have not proven effective, whereas various testosterone esters and nandrolone decanoate produce oligo- or azoospermia in normal men within weeks or months of continuous high-dose exposure.
This has been most extensively studied with testosterone enanthate. A clear decline in sperm concentration is observable for normal men receiving at least 50 mg/week (Figure 6.3); 300 mg/week does not further reduce the count in men who do not suppress at 50 mg/week (Matsumoto, 1990), but fertilizing capacity is also reduced at 100 mg/week (Matsumoto, 1988). Because the major portion of the testis is composed of seminiferous tubules and developing germ cells, this reduction in the population of developing germ cells decreases testicular size by a measurable 15 to 35% from baseline.
Because the normal cycle of sperm development from spermatogonia to mature spermatid in the testis is about 2 months, it is not surprising that the repopulation of the germinal epithelium to pretreatment sperm counts following cessation of steroid administration may take 6 months or even nearly 1 year for some men (Paulsen et al., 1982); there is hope that some androgens with long halftimes will have an even more extended effect.
A large multicenter trial sponsored by the World Health Organization has now demonstrated that long-term testosterone enanthate administration is effective as a male contraceptive in carefully screened males. The mean time for individual subjects to recover to their baseline geometric mean from azoospermia following more than 1 year of weekly 200-mg injections of testosterone enanthate in this study was 6.7 months (range 6.2 to 8.7 months).
The popular press has caused confusion about the reversibility of androgen-induced sterility, and like the confusion about the effects of steroids on blood pressure, this confusion appears to originate from the ACSM (1987) position statement on steroids. This statement refers to an early study in which prisoners were given estrogens and progestagens developed for female contraception, and sperm counts and testicular biopsy specimens were reported to be below baseline values after several months of recovery time
There are several problems with using this report to suggest the possibility of a permanent sterility with androgen use. First, there was enough uncertainty in the interpretation of these data that one of the authors added a dissenting comment in the same journal stating his view that some of the changes reported for testicular biopsies “failed to reveal any change of real consequence” and doubting the accuracy of the semen analyses. Andrologists who have undertaken subsequent studies have been careful to take into account the wide day-to-day variability that is observed in semen quality, and this includes using geometric means of multiple samples. Second, the anabolic steroids tested by Heller et al.
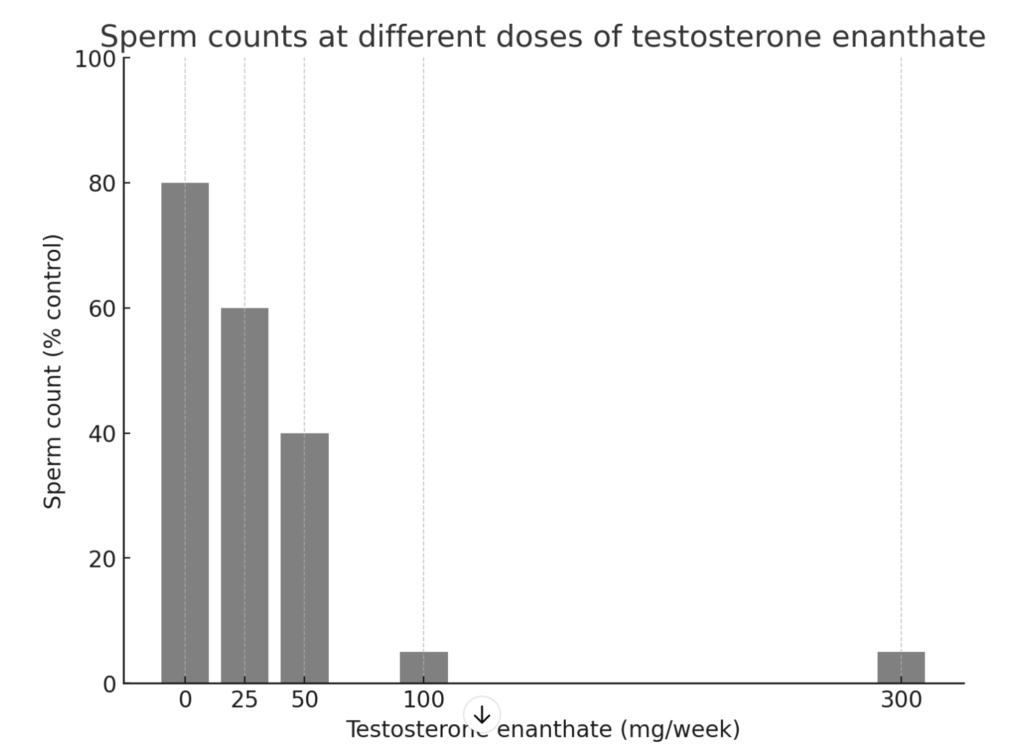
Sperm counts, expressed as a proportion of individual baseline values, at different doses of testosterone enanthate administered weekly by intramuscular injection for 6 months.
(1959) are not those that athletes are generally known to be using; in fact, the closest relative tested was the androgenic progestogen norethandrolone, and this has not been reported to be used by athletes. Finally, none of the authors of this study suggested that the effects might be permanent and no studies since then have made such a suggestion.
Spermatogenic Rebound With Cessation of Steroid Administration
High-dose androgens have also been administered to restore fertility in men with low sperm counts, through a well-recognized but poorly understood rebound that occurs following several months of high-dose androgen sperm suppression . Up to 60% of patients with below-normal spermatogenic activity but otherwise normal seminiferous epithelia show at least temporary improvement in their sperm counts, and some patients show permanent improvement. Norethandrolone, testosterone esters, and mesterolone have all been used in rebound therapy, and some researchers claim that these drugs improve pregnancy success rates. Other approaches to treatment of male infertility have included administration of mesterolone or testosterone undecanoate to oligospermic men in an attempt to support spermatogenesis.
Gonadotropic Relation
The reduction of sperm count is primarily mediated through the suppression of gonadotropins (LH and FSH), although there may be some direct effects on the testes as well. This gonadotropin suppression has been well demonstrated in many of the contraceptive studies as well as in at least one detailed assessment of self-administering athletes.
Earlier studies have suggested that orally active mesterolone does not suppress gonadotropins at doses that elicit androgenic effects and that 17-alkylated androgens also may not suppress gonadotropins at moderate doses . Some steroid-using athletes administer human chorionic gonadotropin (HCG) during or at the end of their steroid cycles with the intention of preventing the reduction in activity or restimulating the testes to a more rapid recovery.
Some evidence indicates that this will maintain testicular function during steroid use, but this may require more careful dosing than self-medicating athletes are likely to achieve. The testes were not fully responsive to a single dose of HCG in athletes treated 3 weeks after the ends of their cycles of steroid use, whereas repeated HCG treatments actually desensitized the testes to LH stimulation . The main risk that athletes run in this use of HCG is an increased probability for the development of gynecomastia.
Binding Protein Effects
Sex hormone-binding globulin (SHBG) is reduced by both 17-alkylated androgens and the esters (Friedl et al., 1991), but the 17-alkylated androgens are more potent in this effect, reflecting either the difference in androgen/estrogen balance produced with these two classes of androgens or the difference in direct hepatic actions of these pharmacological preparations.
SHBG is also reduced in steroid-using athletes, which leads to an increase in free and albumin-bound testosterone. The significance of this change is uncertain because many of the synthetic androgens have a reduced binding affinity to begin with and will be little affected; however, we can predict that a diminished SHBG level will result in a higher clearance rate for testosterone and other steroids that are bound by SHBG.
Case Reports of Athlete Users
One report in the orthopedic literature describes two case reports of athletes who, the report claims, demonstrate sustained hypogonadism as a result of their steroid use. This report demonstrates some of the problems encountered with such uncontrolled “studies.” One bodybuilder had used androgens off and on for 4 years and was using high doses of three different androgens until 6 weeks before his work-up for infertility, when he demonstrated a low sperm count, reduced testosterone concentration, and poor response to gonadotropin releasing hormone (GnRH) stimulation.
One year later he still demonstrated a poor response to GnRH stimulation; however, the report did not verify that he had discontinued his steroid use. This is important, because I have encountered a similar case in which the husband was willing to let his wife go through a complete series of infertility tests before he would admit that he was still using anabolic steroids. The second case cited by Jarow and Lipshultz (1990) was a 39-year-old competitive weight lifter who had fathered three children and now complained of decreased libido; he also had a history of epididymitis.
He was found to have a reduced testosterone concentration but normal gonadotropin levels, and one semen analysis was within normal ranges. The report provided no details about this patient’s treatment including whether or not he received a prescription for steroids. The authors reported these two cases to highlight “the potentially permanent deleterious effects of anabolic steroids to the hypothalamic-pituitary-gonadal axis” (p. 431). These case reports illustrate several key problems that recur in this case report literature. The cessation of steroid use was not verified, the pre-steroid-use clinical status was unknown, and the clinical testing was inadequate for any conclusive diagnosis.
Conclusions
From the evidence of studies of androgen administration, it is not readily apparent that we can attribute significant adverse health effects to androgens as a general class; however, the 17-alkyl-substituted androgens have certain established consequences, all involving the liver. The 17-alkylated androgens produce a consistent and substantial reduction in HDLC/LDLC fractions, possibly increasing the risk of heart disease, although this outcome remains to be demonstrated in androgen users.
Cholestatic jaundice has been observed in frequencies ranging from none to 17% in various categories of patients treated with 17-alkylated androgen, but this condition is readily reversed when androgen treatment is stopped. Peliosis hepatis is clearly associated with use of 17-alkylated androgen but with unknown frequency. Hepatic tumors are rare in men but occur with a frequency as high as 1 to 3% with 17-alkylated androgen treatment, with a latency of 2 to 30 years.
Nearly half of these discovered tumors rupture, although a larger proportion of benign disease may remain undetected. In two cases, including one of a self-medicating bodybuilder, rupture proved fatal.
In contrast to the orally active androgens, androgen esters produce few reports of adverse effects, even though the clinical use of these injected androgens appears to be widespread. This is the basis for their use in male contraceptive trials (World Health Organization Task Force, 1990). However, several case reports involving death or significant illness in athletes self-administering androgens suggest the possibility of other adverse effects that have not been commonly associated with androgen doses in the clinical range. Foremost among these reports are the three cases of stroke reported in bodybuilders and a fourth in a hypogonadal man, who self-administered high doses of androgen.
Because there is no established steroid dosing that can be recommended to produce desired competitive advantages of increased strength or increased aggressiveness, athletes use doses and steroids with no defined upper limit. This is substantially different from the approach used in the development of male steroidal contraception, for which the lowest effective dose has been carefully determined (Matsumoto, 1990). We may speculate that more serious side effects such as thrombotic stroke occur at very high doses, even with androgen esters, through estrogenic metabolites or by crossover interactions with nonandrogenic receptors.
Researchers have speculated that suppression of immune function is a possible consequence through crossover interaction with corticosteroid receptors, although the only study that has examined immune function in androgen-using athletes found an enhancement of immune function (primarily enhanced natural killer-cell activity) in the steroid users. These higher dose effects may only become apparent with prospective study of androgen abusers, that group with no scientifically determined steroid dosing rationale and, especially, with no dose upper limit. Based on case reports of adverse effects, this group may comprise primarily bodybuilders.
Clearly, 17-alkyl substitution in an androgen introduces properties producing health risks that should not be ascribed to androgenic actions, and other nonandrogenic health consequences will occur through the use of black-market preparations of uncertain quality and composition. Other distinctions are emerging even between androgen esters, which suggest that testosterone esters, indistinguishable from endogenous testosterone after the compounds are hydrolyzed in circulation, are potent androgens possessing the fewest short-term health risks at high doses of up to 300 mg/week for at least several months. On the other hand, there is reasonable suspicion that prostatic carcinoma is linked to androgen excess.
The bottom line is that an athlete would be foolish to conclude that there is a safe way to use anabolic steroids; although no disease of androgen excess has ever been described for men, the long-term consequences of androgen supplementation have not been investigated and are simply unknown.






